Is there a positive side of a NEGATIVE PREDICTIVE VALUE?
In previous studies published by Dr. Rache Simmons in NY and Professor Gordon Wishart in Cambridge it is mentioned that te Digital Infrared Analysis has a High Negative Predictive Value.
Personally I proved this same statement. That is :
A SUSPICIOUS LESION "NEGATIVE" OR WITH A VERY LOW SCORE IN THE INFRARED SPECTRUM IT IS MOST LIKELY TO BE NEGATIVE FOR CANCER ON THE FINAL PATHOLOGY REPORT.
Standard recommendations based on the BIRADS system define that a biopsy should not be delayed or postponed specifically in BIRADS IV and V.
BIRADS IV is the most "tricky" from 5%-90% possibilities of being positive. It is the least specific for breast cancer. And yet that is how we proceed.
And even ONLY with a CLINICAL suspicion regardless of the image studies is ENOUGH to recommend a Biopsy.
So then , WHY SHOULD I PERFORM AN "EXTRA" procedure if my suspicion is enough to recommend an Histological Confirmation or BIOPSY?
THE ANSWER IS SIMPLE : BECAUSE INFRARED IMAGE HAS A MEANING AND A PREDICITIVE VALUE.
Case : 38 year old Female , being surveilled for an Upper External Right Breast Nodule known for about 18 months
No previous or personal History relevant for Breast Cancer ( As 90% of the patients assisting to a Breast Clinic)
on PE:it is defined clearly a palpable lesion around 1.5 cm , hard that moves easy , no skin signs , no nipple discharge , ipsilateral negative axillae.
Previous Conventional Standard Diagnostic Images:


Bilateral Mammogram : Dense Breasts : 38 year old patient
( Tough Detection ) , yet with an upper signal pointing out the clinically suspicious area.


Close Up : Undefined Dense Nodule

BIlateral Inflammatory Lymph Nodes

Ultrasound :1.1 cm lesion , irregular in one view and with augmented vascularity on Doppler .
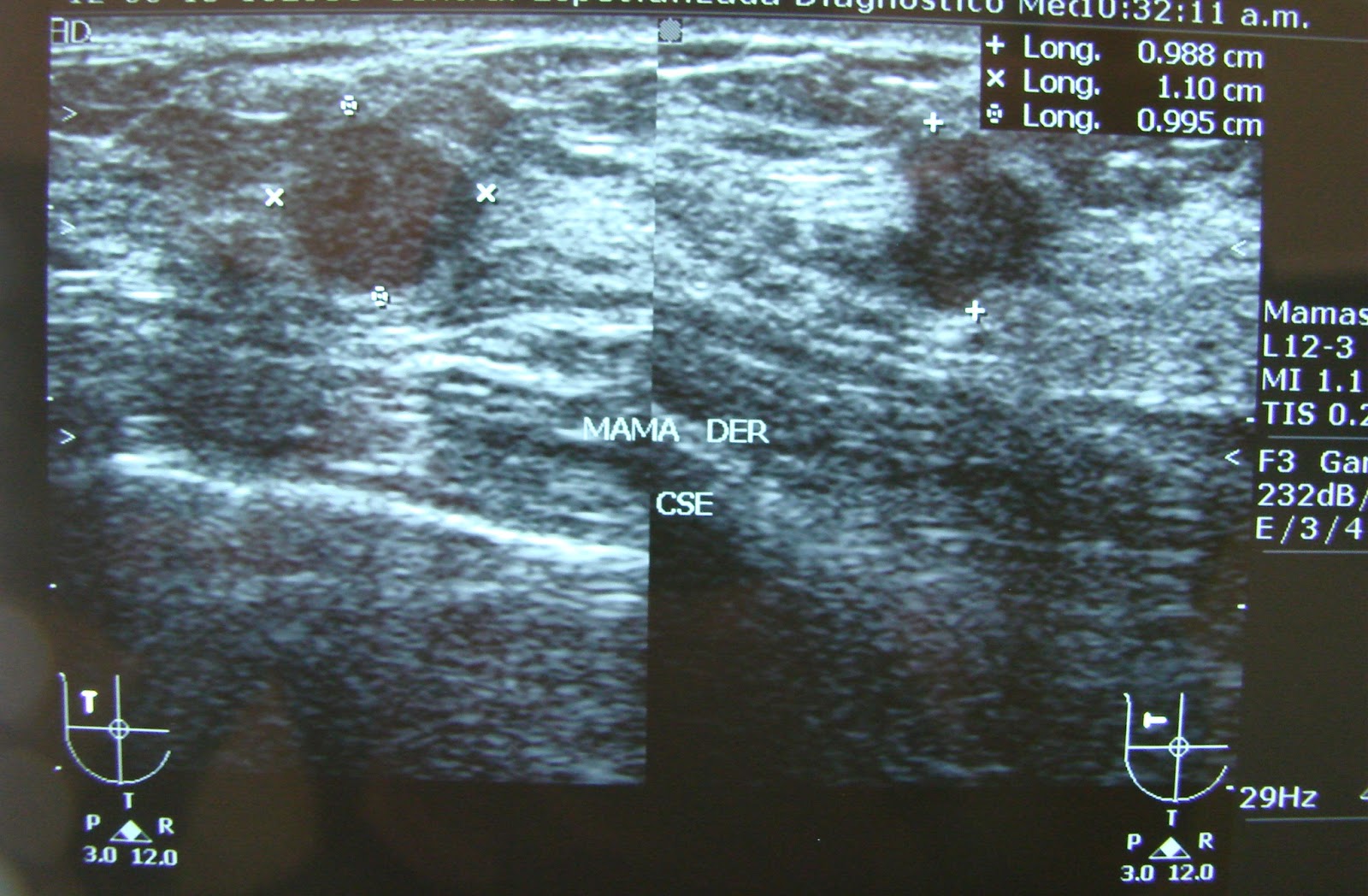
Now the Radiology Diagnosis is a BIRADS IVa Lesion ( previously BIRADS II ) , enough to recommend a biopsy (Low probability) Yet her ObGyn performed a FNAB : 
ATYPICAL NEOPLASTIC CELLS.
Patient is refered to Oncology WITH a clear idea of being dealing with a BREAST CANCER.

ATYPICAL NEOPLASTIC CELLS.
Patient is refered to Oncology WITH a clear idea of being dealing with a BREAST CANCER.
Related Stress facing a BIRADS IV or V is a COMMON CLINICAL SCENARIO in the Breast Clinic. Even some patients present an Important Psycological Trauma.
As a complement study : Digital Infrared Analysis was performed previous to Biopsy , with the following findings.

Comparative Analysis of Both Breasts. Arrow: Clinically PALPABLE lesion , "invisible" for the INFRARED.
Negative Predictive Value : PEACE OF MIND.

Symetrical highest Fucntional Hyperthermias after the Cold Stress Test ( Cold Air) , Lesion at 9hrs of the right Breast : Absent or Invisible.
For some "negative" for the infrared analysis , for me a IR Score less than 100.
Final statment in my practive : Although we have enough (Clinical , Radiological and from Citology )information for a complete removal of the lesion we do know that your nodule is LOW in METABOLISM , LOW in AGGRESIVENESS even if positive for breast cancer , and MOST LIKELY : NEGATIVE FOR BREAST CANCER.(85% or more chances)
"So independently of the final results , you should be OK , you will be OK because the Odds are with you"

Comment : Final Pathology report : Simple Ductal Hyperplasia and a Benign Fibroadenoma.
The Best ANATOMICAL image procedures in Breast are and probably will ever be : MAMMOGRAM(Rx) and ULTRASOUND , the routine combination of both offers an adequate detection (when properly recommended).
Frequency and Initial Age for Screening are constantly being reviewed and are different for different Organizations and even differ between Countries.
ANATOMICAL definition depends on individual THRESHOLDS , and sometimes it is not clear enough in DIAGNOSIS , that is suspicion for Cancer : BIRADS IV(a,b or c) has the widest range of probability for breast cancer : 5-95%
And even FNAB results : in this case Atypical Neoplastic , for some pathologist could represent POSITIVE for Breast Cancer .
And abscence of malignitiy in a FNAB does not rules out 100% Malignancy.
That is why some centers do not recommend it.
A PHYSIOLOGICAL study like the Digital Infrared Analysis of the Breast offers aditional useful information of the clinically interest area.
Its NEGATIVE PREDICTIVE VALUE : Low score or "invisible" , non identified in the infrared specturm is strongly related to Abscence of Malignancy , or better yet as a complementary study means in this case :
LOW or NULL METABOLIC RATE
"The DIRA of the Breast Shoul Be Routinely performed as a complementary Metabolic Procedure to Anatomical Standard Images and restricted to Certified Specialists in Breast Pathology : Oncologists , Radiologists , Breast Surgeons and Oncological ObGyn."
"Prospective controlled protocols would confirm this findings. "
EMC
















