Great week you all ..!
Last night I was having a look at my Blog's statistics.
And I reached the conclusion that the sample case with more hits was:
BIRADS III and Infrared......
So I must think that although you do not comment at all (who would , this issue is too controversial even to speak about it....)
I sense that the majority of my readers should be breast cancer specialists ( radiologists , oncologists, Gynecologists or breast surgeons)
If I am right you can have a smile at home!!!!
Well keep in touch........BIRADS III , to BiRopsy or not to BiRopsy. ( Visit and or Join The BIRADS/Infrared Project)
at:
A promise is a debt :
A few year ago a 40 years of age asymptomatic patient of mine underwent an screening mammogram and handled this images:
Medio Lateral Oblique view , evident density assimetry in the upper outer right quadrant.
Close up : No Microcalcifications are seen , yet I might agree retrospectively you can argue architectural distorsion and irregular profile. BIRADS 0 went to a complementary Ultrasound:
An heterogeneous Morphological Lesion is found , with cystic and solid components almost circular in its form no posterior "shadow" is seen .
FINAL RADIOLOGIC DIAGNOSE BIRADS III , close follow up right?
I WOULD THINK SOME MAY ARGUE AN ERRONEOUS OR MISTAKEN DIAGNOSIS , YET IT HAPPENED.
Then she attended 3 months later to a SECOND Opinion.
So this are her DIRA images:
 Basal DIRA series , anterior and oblique views , upfront as any NEW language or Unknown one there should be a little doubt an distrust.
Basal DIRA series , anterior and oblique views , upfront as any NEW language or Unknown one there should be a little doubt an distrust.
If you look up closely actually there is a little assimetry that depends on the upper outer quadrant of the Right Breast what we might call THE INTEREST AREA or IA.
After cold challenge the Functional or Physiological series were taken. No obvious difference for the UNTRAINED eye.
Yet with the Software "Isotherm" application a Slight difference is then seen in comparison to the left side (ARROW) it actually is coincidental to the physical finding of an "irregularity" zone at palpation .
Same image but different color option.
So now I am thinking :" there is a HIGH METABOLIC area that is coincidental with my MORPHOLOGICAL findings by standard mammogram and ultrasound. Not to mention that this area by incidence is the highest for a Breast Cancer to appear." EMC
Recommendation : I think you should perform not in 6 months but
as soon as possible a Mammography and corresponding ultrasound.
These are the images taken :
Cefalocaudal view , density assimetry now is evident.
Oblique view , confirm previous findings.
Close up : Highly suspicious Microcalcifications are NOW EVIDENCED
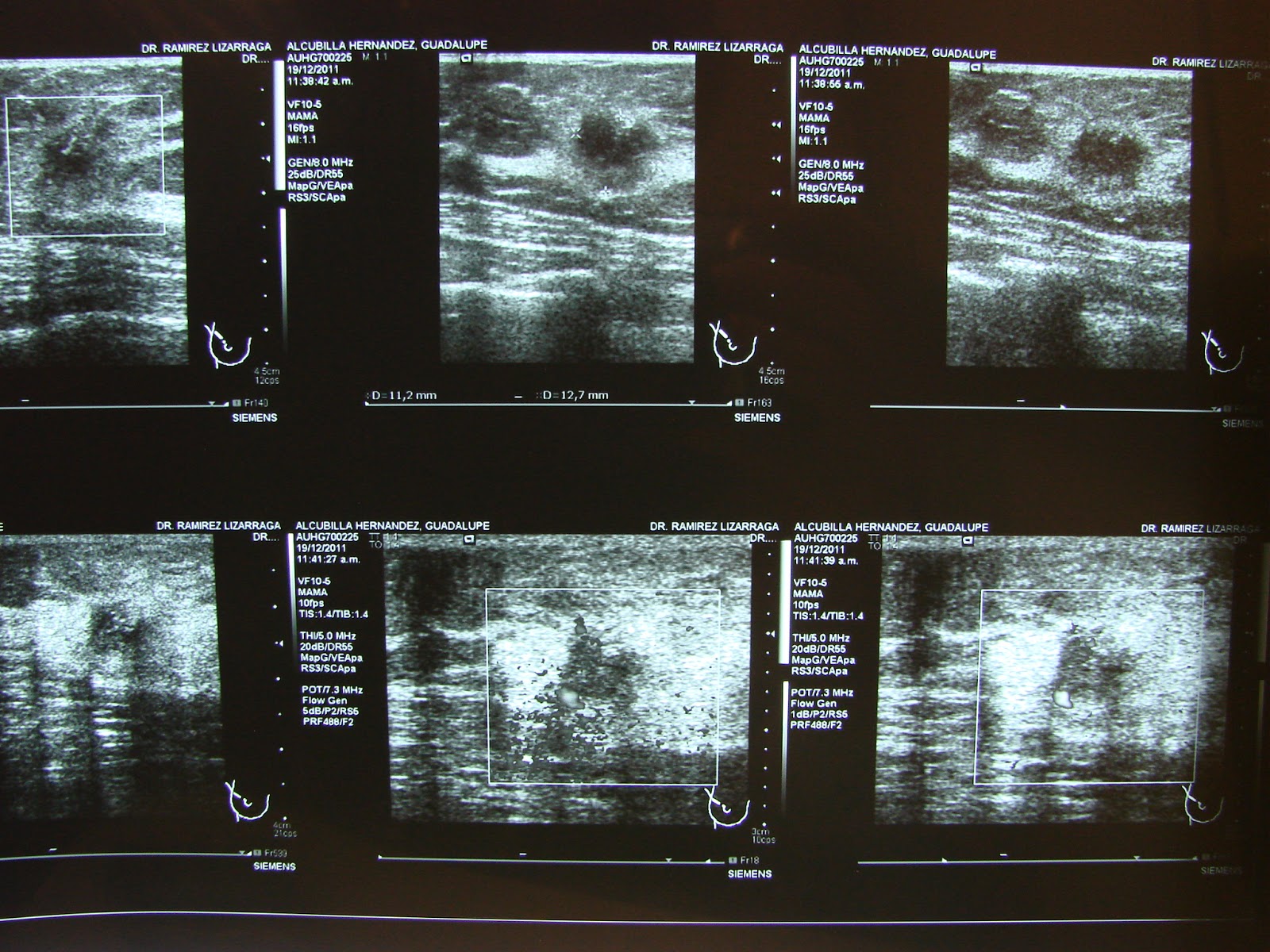
Corresponding Ultrasound Images : NOW MORPHOLOGICAL CLEAR CHANGES ARE SEEN AND DOPPLER DEMONSTRATES INCREASED VASCULAR FLOW.
BIRADS V .....
Most would argue that based on experience diagnosis could have been different previously. Better yet if there is a Close Surveillance the same diagnostic algorithm would have been done. And even if DIRA proofs a benefit in helping DIAGNOSIS and DETECTION , prognosis would be the same.
Reality : BIRADS III is based on INDIVIDUAL RADIOLOGIST Criteria , Follow up sometimes cannot be achieved.
And BIRADS II was another possibility for the first classification.
The ecuation is simple:
"BIRADS III (even IVa) Morphologically proven , DIRA coincidental for HIGH METABOLIC ACTIVITY Plus ONCOLOGICAL experience : Recommend for SURE to Biopsy."EMC
These are the images taken in the OR , a possible next level.
Keep in touch.............
The idea is to gather BIRADS III lesions internationally , I will creat this next blog for those who would like to participate......
But now I am going to celebrate my Boy´s Birthday so I guess we will see you around next week.
http://birads3infraredproject.blogspot.mx/




 She underwent lumpectomy and Sentinel Lymph Node disection , Chemotherapy Radiotherapy and Tamoxifen as Hormotherapy , NOW :
She underwent lumpectomy and Sentinel Lymph Node disection , Chemotherapy Radiotherapy and Tamoxifen as Hormotherapy , NOW : 





.JPG)
.JPG)
.JPG)








.JPG)





























{kind=link}