Would you like to see an Example??
Early 40´s asymptomatic woman , first mammography screening.
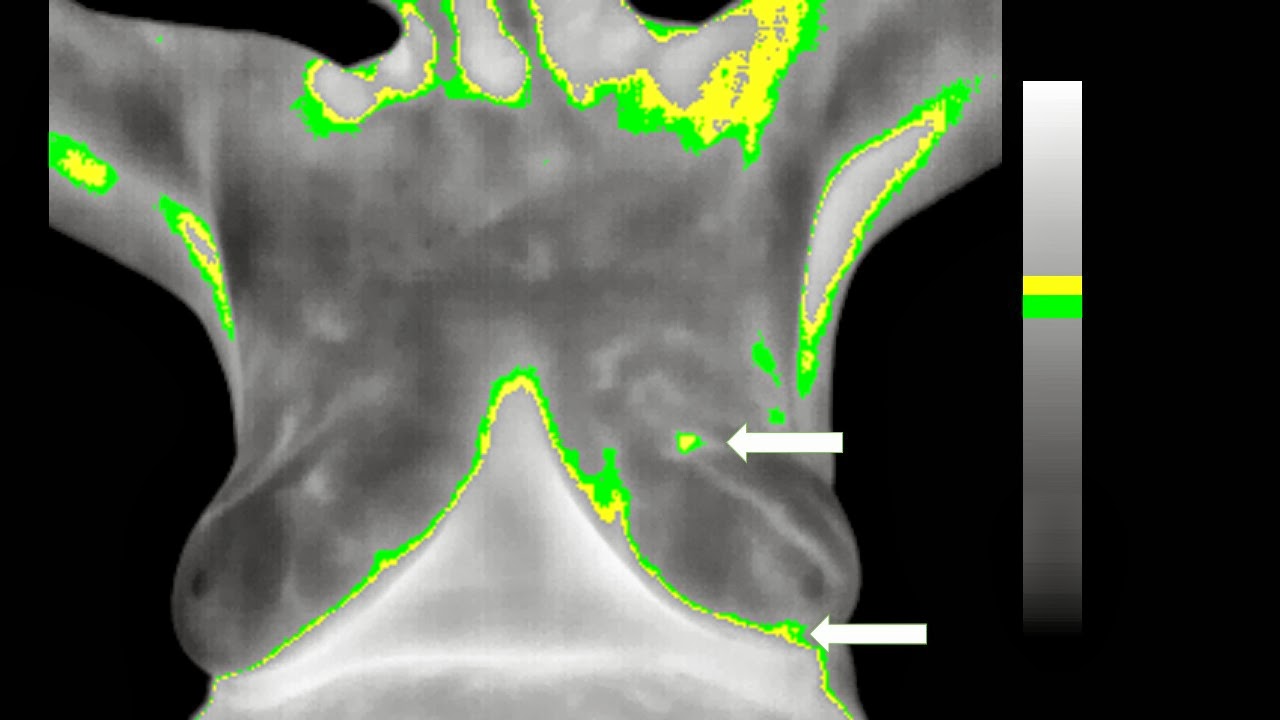
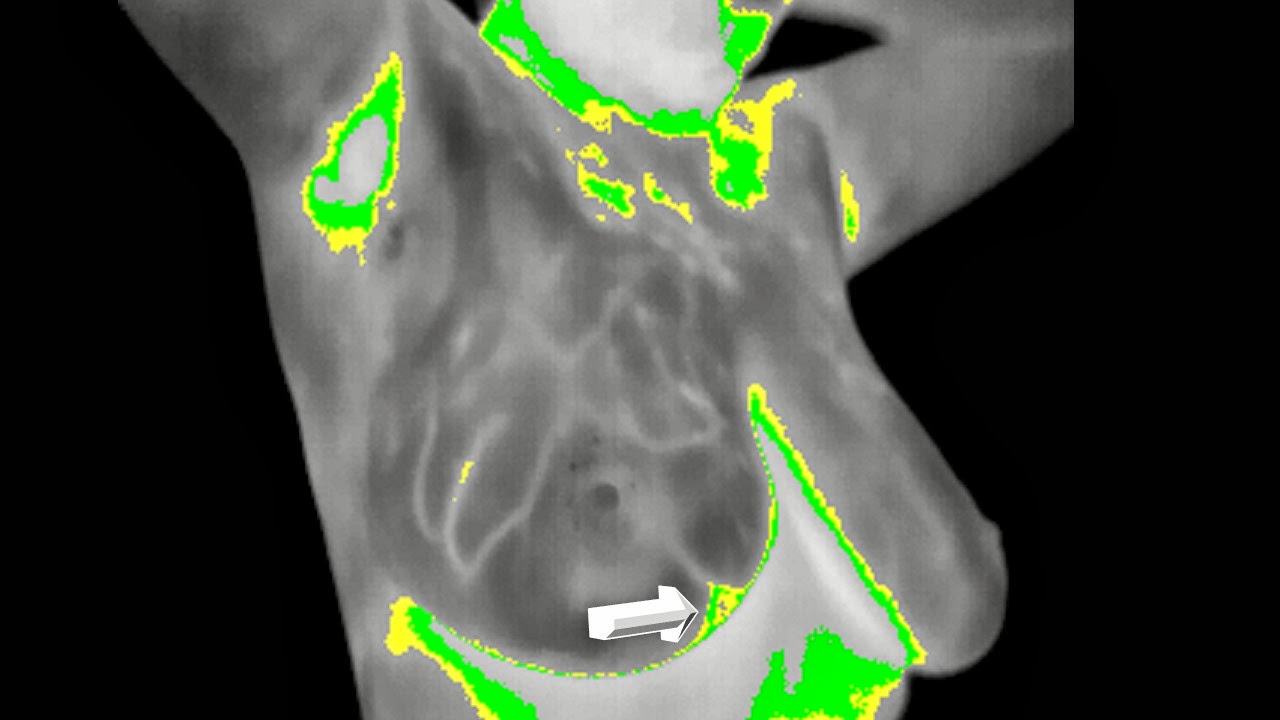
On Physical Examination after the images an irregular "soft" lump was felt on her right inner upper quadrant......



Anatomically Clearer than this , is Impossible and that is why detection is supported on MORPHOLOGY.
Makes more than sense....
So would you perform an Infrared Complementary Procedure???
Vast Majority : will say ABSOLUTELY NOT....Right?
Well I did , why :
BECAUSE EVEN BEFORE BIOPSY I HAVE USEFUL INFORMATION FOR THE PATIENT TO GIVE.......
METABOLIC INFORMATION....Makes sense to me .....( and to tell you the truth it is brainstimulating......)
"EMPATHY , PREDICTION , COMPLIANCE , STRESS , AND IN SOME CASES EVEN THERAPEUTIC DECISIONS CAN BE SUPPORTED BY AND INFRARED IMAGE."
EMC.
I believe you should learn it TOO.... don´t you think so ???
To see the IR images Keep posted OK??? , have a great week......



























.JPG)
.JPG)
.JPG)
.JPG)







