Simple and easy there is no doubt and Standards are Changing and including by LAW the comment that includes BREAST DENSITY .
Dense breast tissue not only is at risk for more active tissue , but it is obviously a
VISUAL Obstacle for Xray definition.
Even Clinically suspicious as the following case are reported surprisingly as totally benign : BIRADS I
Morphological complement with Ultrasound clearly defines the even palpable nodule , great complement fortunately , enough for clinical decision making ........
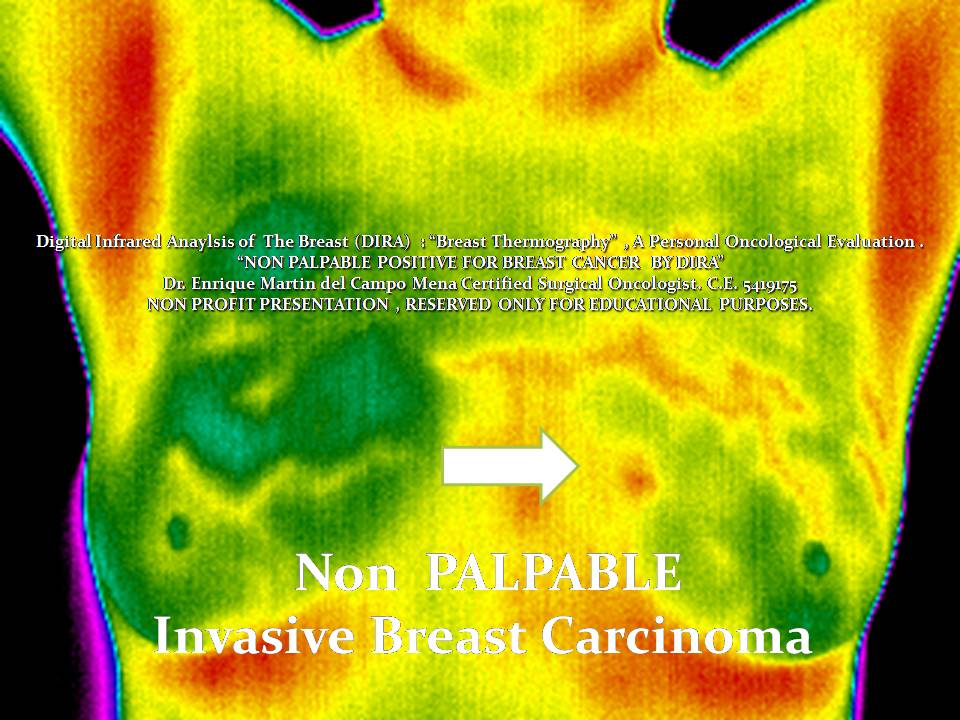
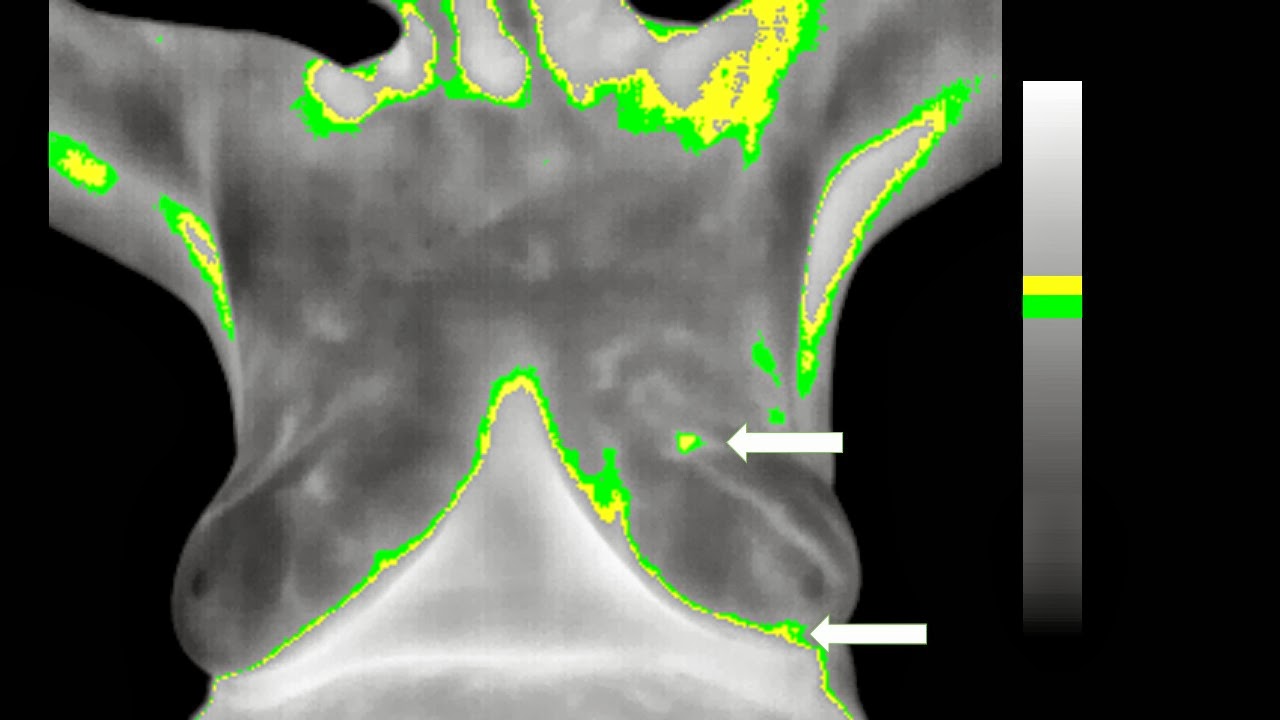
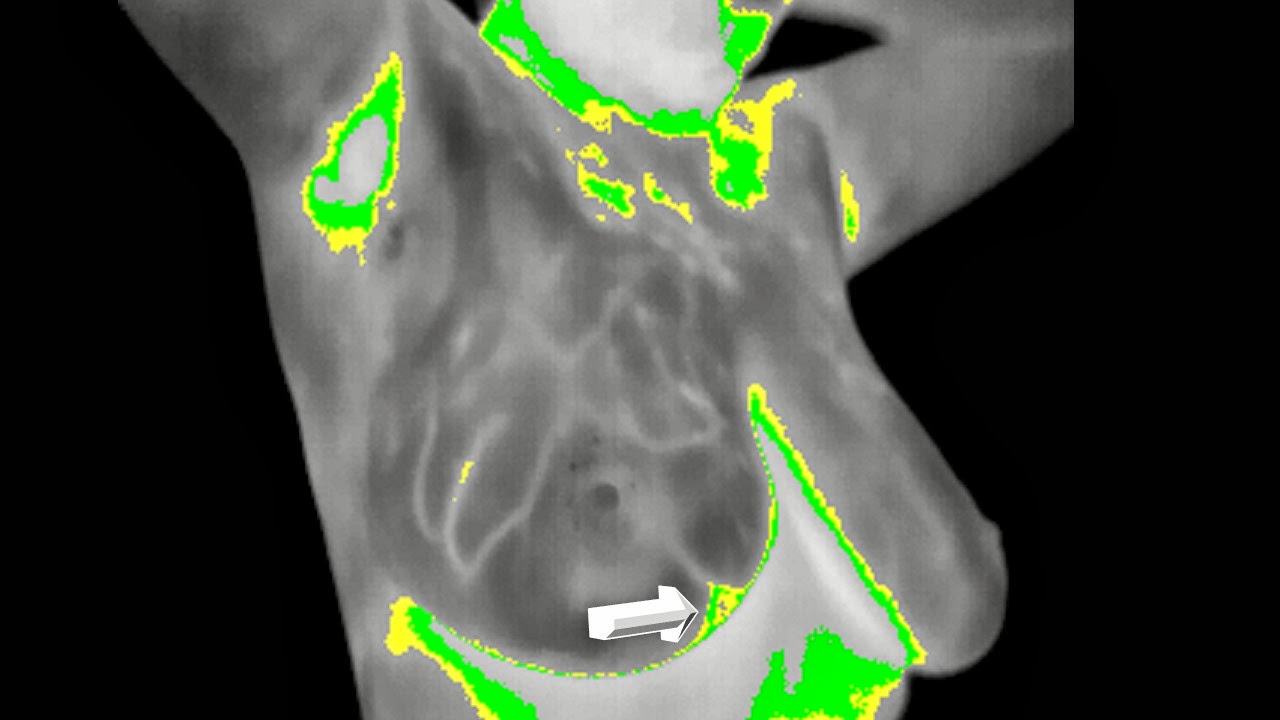
Complementary Digital Infrared Image were these:
Basal Frontal
Basal Oblique Right
Basal Oblique Left Views
Functional Frontal
Functional Right Oblique
Functional Left Oblique
Close up.
COMMENT :
For me there is no DOUBT , Dense Breasts cannot rely only on Mammography , I am guessing everyone agrees.
Complementary procedures are obviously Needed.
Ultrasound when clinically evident is great.
"Infrared when clinically ASYMPTOMATIC , could help guide ULTRASOUND and define :
SUBCLINICAL POSITIVE BREAST CARCINOMAS"
EMC
And you can quote me on that ........
So here is the thing : around 30-40 percent of cases are diagnosed in women 45 years or younger , population defined radiologically as Possible DENSE BREAST .....
That is why even after 40 MILLION mammograms in the US every year 20-30 percent are clinically evident.
And will be , if we do not try anything else...
To include an adaptative strategy for non INVASIVE or IONIZING Screening in these women that are not candidates for Mammography or Have an anatomical BARRIER for Xrays.
It not only MAKES SENSE but it is a true LOGICAL POSSIBILITY.
Think about it and SMILE.
Welcome to open your minds and eyes.....
I think you should give it a try....
See you.


















.JPG)
.JPG)
.JPG)
.JPG)