One of the most frequent arguments Infrared Supporters mention throughout the web is that Angiogenesis that appears in Breast Cancer is able to rise local temperature so that the Infrared Detector could actually see and Measure.........
Is this principle correct?
Is angiogenesis capable of an abnormality enough for it to be seen and recorded?
Oncological Physiology Mentions that Angiogenesis is a determinant factor for some tumors to hold on and then grow.
It seems quite logical , it has been proven and as such we must accept......
Yet Breast Cancer is an Heterogenous Disease , meaning that there are different types of Breast Cancers and that some may not have Neoangiogenic Factors or Enough Microvascular Density.
As a matter of fact the latter is just a weak prognostic factor in breast cancer.... so I believe that Angiogenesis is NOT THE ONLY FACTOR that rises Infrared Radiation from a given Tumor or Cancer.
Yet Breast Cancer is an Heterogenous Disease , meaning that there are different types of Breast Cancers and that some may not have Neoangiogenic Factors or Enough Microvascular Density.
As a matter of fact the latter is just a weak prognostic factor in breast cancer.... so I believe that Angiogenesis is NOT THE ONLY FACTOR that rises Infrared Radiation from a given Tumor or Cancer.
Nevertheless I will present a clinical finding that supports the principle of angiogenesis and Infrared Detection........
Sample Case :


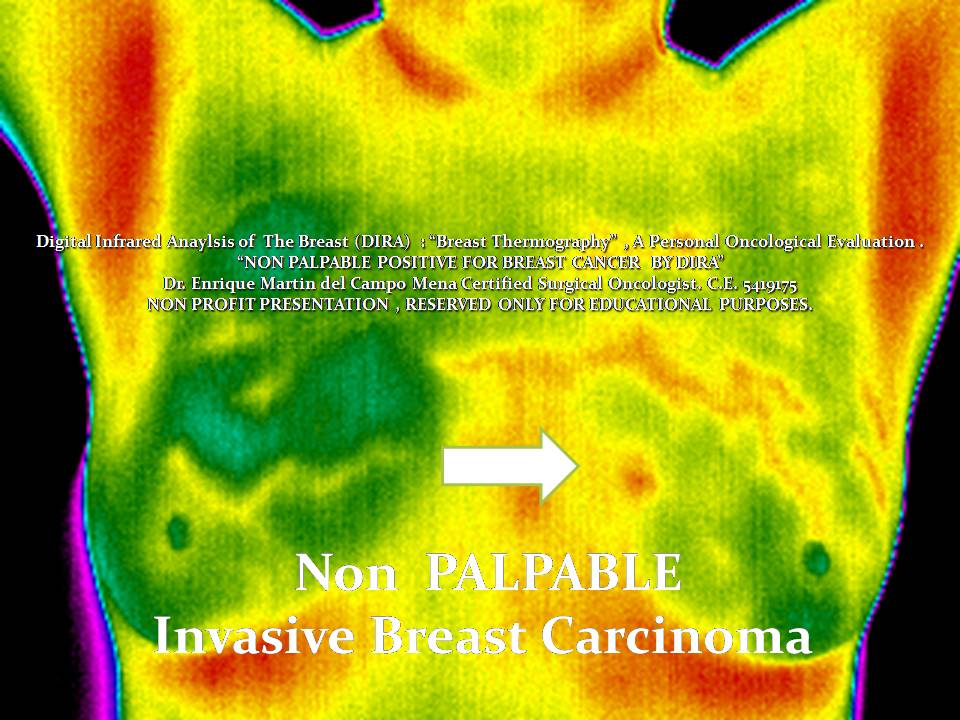
Infrared Analysis of the Anatomical Region. Clear Differences in Color are seen as Infrared Radiation Rises. Advanced and current State of the art IR detectors have a LARGER color scale, resolution and pixels.

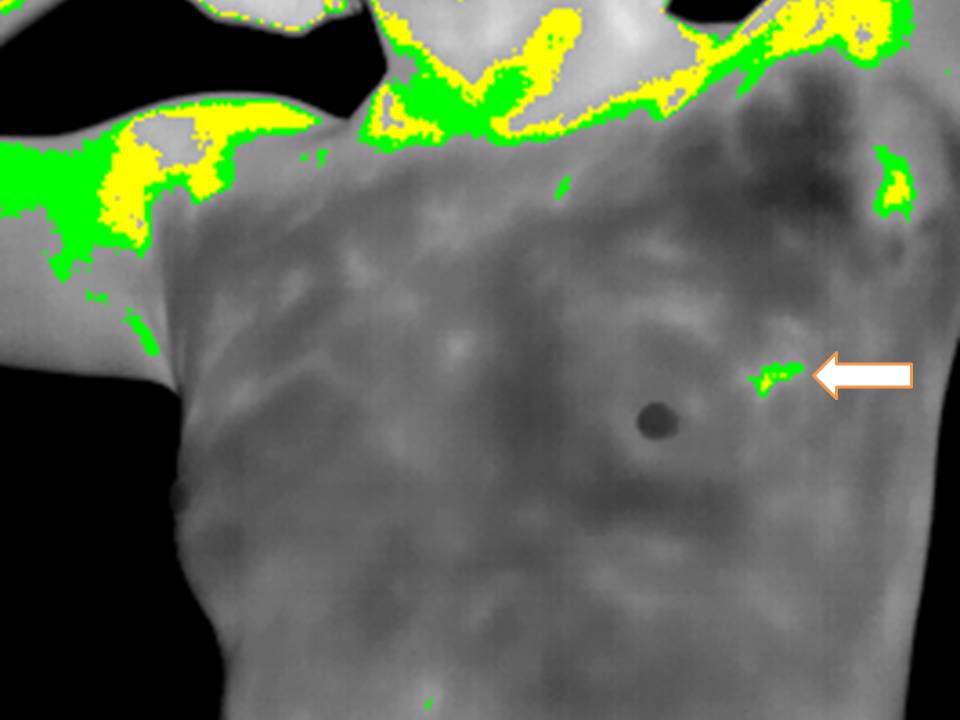
Software Color and Palette options can can choose only gray scale , white and black:
 And with the Use of Automatic "ISTOTHERMS" or color ranges , the highest IR radiation areas are limited and subsecuently could be measured.
And with the Use of Automatic "ISTOTHERMS" or color ranges , the highest IR radiation areas are limited and subsecuently could be measured.

Software manipulation and applications can give objective numerical reproductible results and hence record them and compare if future instances occur.
Angiogenesis in Angiosarcoma is EVIDENT , local heat is risen because of VASCULAR DENSITY and in part I assume could explain what happens in SOME TYPES of Breast Cancer.
If this should be enough to be present at Breast´s Skin Surface and be a CLEAR sign that actually means malignancy is for Prospective Controled Clinical Protocols to be defined.
IR Analysis is related to metabolic , inflammatory , infectious and vascular biological conditions of the focused area.......
These images Mean NOTHING to Most Common clinicians and or Oncologists , they do not change their treatment algorithm or way to make a diagnosis , are useless , time consuming and considered fraudulent........
Are they really?
But they proof at least ONE Physiological and Pathological principle : Angiogenesis.
Time to think..........

Female patient in her early 40´s, previous history of RADIATION Therapy in her Right Thigh during childhood for a Liposarcoma more than 25 years later Metachronic ANGIOSARCOMA , Treated in the US , with chemotherapy , surgery and TRAM FLAP plus radiation , yet clinical evidence for Recurrence a year after being in control .
Infrared Analysis just to have an simple image:

Infrared Analysis of the Anatomical Region. Clear Differences in Color are seen as Infrared Radiation Rises. Advanced and current State of the art IR detectors have a LARGER color scale, resolution and pixels.

Software Color and Palette options can can choose only gray scale , white and black:


Software manipulation and applications can give objective numerical reproductible results and hence record them and compare if future instances occur.
Angiogenesis in Angiosarcoma is EVIDENT , local heat is risen because of VASCULAR DENSITY and in part I assume could explain what happens in SOME TYPES of Breast Cancer.
If this should be enough to be present at Breast´s Skin Surface and be a CLEAR sign that actually means malignancy is for Prospective Controled Clinical Protocols to be defined.
IR Analysis is related to metabolic , inflammatory , infectious and vascular biological conditions of the focused area.......
These images Mean NOTHING to Most Common clinicians and or Oncologists , they do not change their treatment algorithm or way to make a diagnosis , are useless , time consuming and considered fraudulent........
Are they really?
But they proof at least ONE Physiological and Pathological principle : Angiogenesis.
Time to think..........






.JPG)
.JPG)
.JPG)
.JPG)
.JPG)


.JPG)
.JPG)













.JPG)
.JPG)
.JPG)