BEST WISHES FOR 2013.
We Oncologists , ObGyns , Radiologists , Breast Specialists and Generally all Women and Population Believe and KNOW that the SMALLER the Tumor is The BETTER the prognosis.
Anatomical definition of Mammography sporadically (in my experience) detects invasive tumors less than 1 cm.But I am guessing , correct me if I am wrong , that most international breast specialists have little experience in SMALL tumors.
So , prognosis is related directly to small size and viceversa..
Mammography STRENGTH around 50 to 69 years is such that would be useless to recommend anything else , or even try to atttack its controversies , flaws , overdiagnosis , pain or possible radiation damage.
I support firmly Mammogram for detection in this specific group .
YET AROUND HALF THE BREAST CANCER POPULATION IS 50 YEARS OR LESS.
In this setting STATISTICS and BENEFITS of Screening are in doubt or have not changed at all after 30 years (40y and less) , mainly because BREAST DENSITY
Optimal Screening Coverage in developing countries differ enormously it ranges below 10% when we know that the ideal percentage is around 70 and a minimum of 10 years of continuos screening .
Even more , its recommended Frequency is in review and different recommendations occur internationally.
I believe THE COMMON ENEMY IS CANCER , to add a possible tool against it means no harm and should not be rejected. The NEW benefit of the doubt should overcome . In order to learn its meaning and possible applications it is a TASK meant for ALL.
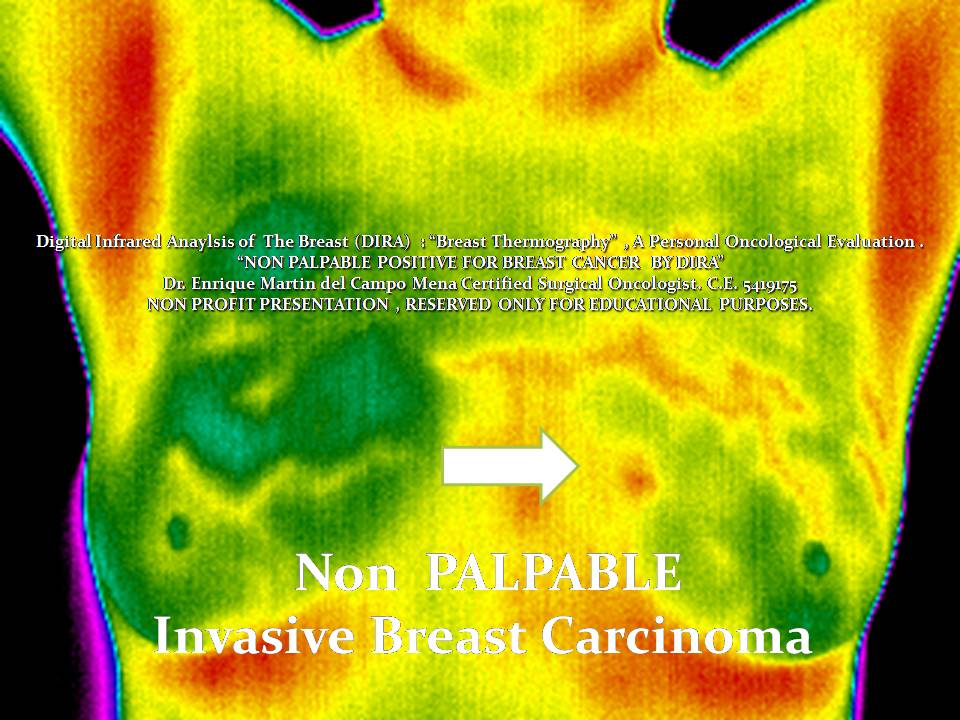
So lets begin 2013 with this specific scenario : NON PALPABLE LESIONS that are visually detected by the DIGITAL INFRARED ANALYSIS.
By NO MEANS i recommend (for now) as a substitute for a Mammography , this images images represent a small piece of my Universe , only if a Mulcentric research in developed countries would be involved this piece of evidence could be reproduced.
They are MEANT TO BE the cornerstone for future research.
What should we do between Mammograms (2 or 3 year) changing intervals?
You should be the judge.








I Know it sounds RIDICULOUS or even ABSURD , believe me I started with the same doubts and rejection. After all I was not even told during my Oncological Training that this could be possible.
Yet this images are the result of a Blinded Challenge in order to Stablish if I could recognize the presence or abscence of the detected lesion ( ALREADY BIASED) I should mention.
Yet , for me it is Very Clear , Assymetry , vascular network and persistent Hyperthermias after the cold Challenge , plus axillary temperature and possible mammary fold characteristics
(EMC Infrared Pentad for Breast Cancer )
REPRESENT A HIDDEN CLUE OR LANGUAGE FOR INVASIVE BREAST CARCINOMA.
Obviously THIS IMAGES HAVE TO BE be redefined and reconfirmed .
But :
IF THEY ARE CONSTANT for 1-2 cm NON PALPABLE INVASIVE BREAST CANCER.Specially Aggresive forms : Grade 2 , 3 or HER2neu+++.
My Hypothesis is that DIRA could actually Help Detection , Downstage Breast Cancer Statistics and most of all Help Women.
Digital Infrared Analysis of the Breast SHOULD be reexplored and resitricted only to Certified Breast Specialists.
Fortunately there is only one option to confirm if what I was able to Find is true: that would be forward prospective controlled trials to define non palpable breast Cancer under the infrared spectrum and analysis : emartindelcampo@yahoo.com
Have a great 2013..
No hay comentarios:
Publicar un comentario